")
[cmamad id=”22361″ align=”center” tabid=”display-desktop” mobid=”display-desktop” stg=””]
Since 1928, Big Pharma has been covering up studies showing that this natural mineral does more for blood flow and blood pressure than their own treatments…
—-Important Message—-
These 5 Foods Naturally Improve Blood Flow to the Penis
The thin arteries in a man’s penile chambers need to be opened up wide for good blood flow.
And blood flow is important because good erections depend on good blood flow.
When men have good blood flow to their penis, they get more engorged and longer-lasting erections… And erectile dysfunction goes away naturally.
Just recently, I discovered 5 simple, delicious foods that naturally improve blood flow to the penis…
AND these foods also lower men’s blood pressure naturally (and better than Big Pharma treatments).
———-
This Natural Mineral Improves Blood Flow to Your Penis
Potassium’s ability to counteract sodium’s effect on blood pressure has been known since 1928… But this is still largely ignored by the popular press.
The mainstream press gets much of its advertising revenue from food industries…
And the companies that provide the most income always use far more sodium than potassium in their products: General Mills, Kraft, Nestle, etc.
On top of that, media companies are also sponsored by companies in the pharmaceutical industries – or even partially owned by them…
So cheap supplements that lower blood pressure will always be ignored in lieu of pharmaceutical drugs that do the same.
In the 1940s, sodium chloride overtook borax as the most common preservative in foods…
That is when Americans began consuming more sodium than potassium.
This is an inversion of the natural sodium/potassium (Na+/K+) ratio, where the amount of potassium always surpasses the amount of sodium.
Essentially all natural foods, besides seaweed and bananas, have a sodium/potassium ratio of around 1∶7 to around 1∶15.
Even raw beef, perhaps the most sodium-heavy natural food, has a sodium/potassium ratio of approximately 1∶7.
So, how high can we go before it starts to influence blood pressure?
Well, we now have enough published evidence to answer that question.
And the evidence seems to show that the ratio of sodium to potassium matters more than the absolute amounts of each…
And also that a sodium/potassium ratio of around 1∶4 should be fine.
“Our data indicate that when people have an increased intake of potassium, high intake of sodium is not associated with higher BP.”
So if it’s true the ratio matters more than the total amounts of each…
… then it makes sense that simply taking potassium supplements would lower blood pressure just as effectively as “salt restriction.”
Of course, a ratio can always be brought down to any value either by decreasing the numerator (sodium) or by increasing the denominator (potassium).
But on a practical level, increasing potassium is an easier way to lower blood pressure than restricting salt…
And that’s because it’s just far more convenient.
Taking a few grams of potassium each day leads makes salt consumption relatively innocuous…
It renders the salt incapable of influencing blood pressure at any intake level under suicide-sized doses.
The first modern clinical studies demonstrating that potassium could be used clinically started surfacing in the early 1980s:
In this study, the researchers gave 23 patients with high blood pressure 60 millimoles (mmol) of potassium per day – as potassium chloride (KCl).
This corresponds to 2.34 grams of potassium (4.98 grams of KCl).
The participants continued to eat as they had before – and without any consideration of salt intake.
This was a crossover study of one month’s duration.
After that, they switched the placebo and potassium groups and repeated the trial.
This process added more statistical weight to the study – necessary, considering the small number of participants involved.
And they found an undeniable and statistically significant decrease in average blood pressure:
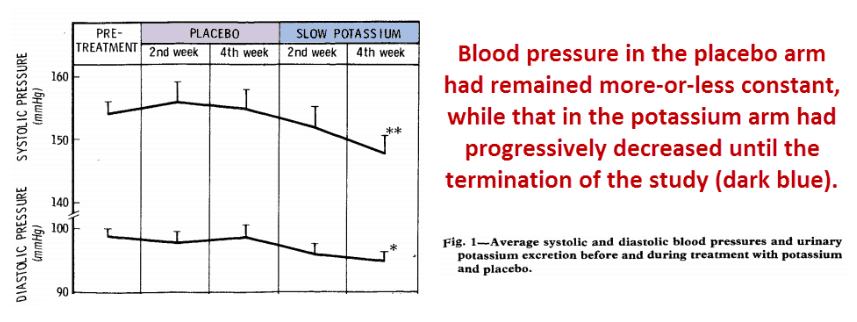
They took a few other measurements. The most notable was an 11.2% increase in urinary sodium in the potassium group.
“All patients who entered the trial completed it without any adverse effects.”
The only other prior comprehensive study that compared blood pressure with potassium supplementation was done in Japan.
[cmamad id=”22362″ align=”center” tabid=”display-desktop” mobid=”display-desktop” stg=””]
And that study also showed a decrease in blood pressure upon potassium ingestion.
This is very practical…
And there are many potassium salts to choose from:
They include potassium chloride, potassium iodide, potassium ascorbate, potassium citrate, and potassium glycinate…
We can take all of these in gram-sized doses safely.
Potassium iodide
Potassium iodide is great for immunity because the iodide ion is a neutrophil substrate…
It converts into the antibiotic/antifungal hypoiodite ion under the action of its myeloperoxidase enzyme.
In the absence of iodide, neutrophils will create less effective hypochlorite ions from chloride atoms.
Iodide is also necessary for the synthesis of thyroid hormones…
So potassium iodide is a good addition to table salt.
“The only other controlled study of potassium supplementation alone in patients with essential hypertension also showed a fall in blood pressure which was greater than that in our study … However, this Japanese study was done on inpatients who were on potassium supplementation for only 10 days and on a sodium intake of 260 mmol/day; potassium intake was increased by 100 mmol/day.”
Potassium ascorbate
Yet perhaps the best solution for most people is potassium ascorbate, which will keep blood pressure in range while also supplying vitamin C.
I think we all know by now that saturated fats and cholesterol do not cause cardiovascular disease…
And Linus Pauling presents a good case for cardiovascular disease simply being a vitamin C deficiency – a type of subclinical scurvy.
There is no reason to take only one type of potassium supplement – and mixing them up might be the best all-around approach.
With these different potassium supplements, you can control your blood pressure while also getting nutrients such as ascorbate, iodide, citric acid, and glycine.
And many other studies demonstrate the reliability of this effect.
Below is another study published just five years later.
They used a 20% lower dose of potassium, but they also ran the trial four times longer:
This study used 37 patients.
That’s more participants than the previous study. But since it wasn’t a crossover design, the two studies are more or less equivalent in statistical power.
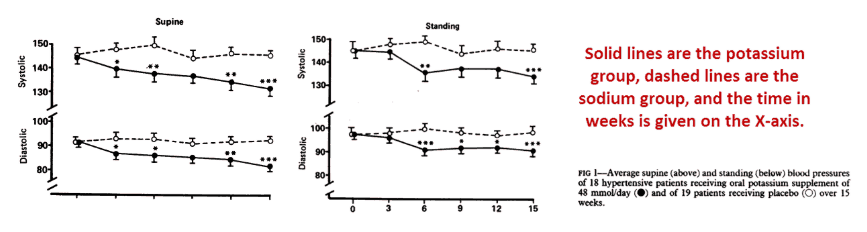
In this study, they gave the patients 48 mmol of potassium daily (corresponding to 1.87 grams of potassium or 10.3 grams of potassium ascorbate).
They demonstrated a dramatic decrease in blood pressure even at this lower dose.
This somewhat stabilized after 15 weeks, yet it does appear to be continuing to some degree…
So this does appear to be a rather consistent effect known since the 1980s – and I’ve yet to see an exception to this rule.
What about hormones?
Catecholamines (these are hormones including dopamine, epinephrine, and norepinephrine) and nitric oxide can also influence blood pressure…
But the sodium/potassium ratio is more fundamental and should influence blood pressure even when accompanied by changes in epinephrine and nitric oxide.
“All patients completed the trial without suffering any adverse effects, and all seemed to comply with the treatment satisfactorily throughout the study.”
Potassium is far safer and much cheaper than synthetic drugs designed to lower blood pressure (e.g. those from Pfizer, Merck, Eli Lilly).
Since these companies make millions off these drugs every year, it’s no surprise that potassium is rarely mentioned as an option.
And there are more (and more) newer drugs available, proving that humans are not evolving fast enough to deal with our increasingly lower potassium intake.
Here is another study:
This study used 59 participants, more people than the two preceding studies.
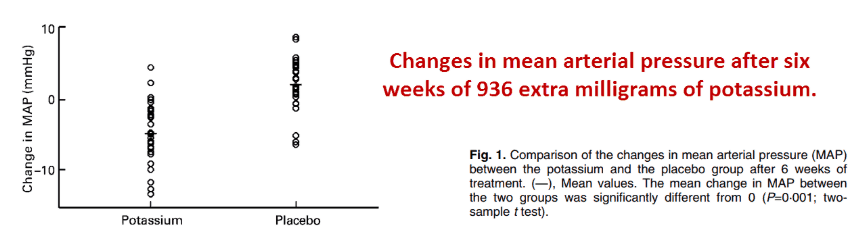
The study lasted for six weeks and used the lowest potassium dose of 24 mmol per day (corresponding to only 936 milligrams of potassium, or 3.98 grams of potassium iodide).
Surprisingly, this study noted a greater change in blood pressure despite the lower dose used.
The mean arterial pressure went down by 7.01 mmHg, systolic blood pressure by 7.60 mmHg, and diastolic by 6.46 mmHg:
They explained this greater effect – despite the lower dose of potassium – by the chloride ion actually counteracting the potassium at higher doses.
They cited three studies showing that the chloride ion was involved in blood…
Yet it is also apparent in this study that the sodium/potassium ratio makes a difference – because potassium chloride was used in all of the aforementioned studies.
And this does appear to have a degree of truth to it.
In one study they cited, 2.76 grams of sodium chloride induced a 5.7% increase in blood pressure.
Perhaps this is not surprising.
But they found absolutely no change in the group that had the equivalent amount of sodium phosphate.
“Evidence from epidemiological studies and clinical trials has indicated that [sodium/potassium ratio] is positively correlated with blood pressure, and that the nature of this association appears to be stronger than that for urinary potassium and sodium alone.”
But there was a quirk to this study: The participants were academics at King’s College London.
Although these people fell within a similar weight and age range as the others, they had a lower heart rate on average.
Catecholamines increase blood pressure through the heart rate…
And the fact that these people volunteered for the study strongly implies a low-stress state.
The subjects in the low-dose potassium chloride group excreted 13% more sodium.
This study is more indication that potassium is more influential the higher your sodium intake is.
And here’s another study…
It showed that when sodium chloride is held to under 6 grams per day, potassium has no effect on blood pressure.
In other words, blood pressure is only related to sodium in people who consume over 6 grams of salt per day.
Stating this in yet another way, potassium can only reduce blood pressure so far… So a very high potassium intake is not fatal.
The Yanomami tribe of Venezuela don’t eat much salt – but they do eat a lot of bananas…
(As we know, bananas contain a lot of potassium.)
And their blood pressure of 104/61 mmHg doesn’t increase with age.
Their sodium/potassium intake ratio has been estimated at around 1∶25 and their sodium/potassium excretion ratio is nearly unbelievable – measured at 1∶100.
Even with a normal potassium-heavy sodium/potassium ratio – such as 1∶5 – people always excrete more sodium because it’s the primary extracellular ion.
Urine with 100 times more potassium than sodium is very rare, and doesn’t happen much outside of banana-eating tribes that totally don’t eat salt.
“In ancient ages, the ingested potassium to sodium ratio was very high, as high as 16:1. Nowadays, the ratio is only 0.65 in the North American population, a value close to the value (0.56) found in our study, confirming the inadequate mineral balance in their usual diet.”
This next study was done on Brazilians, the highest salt-eating country on the planet.
Their average sodium intake is 12.8 grams per day (12.9 grams per day in this particular study)…
So they provide the most striking juxtaposition imaginable against their Yanomami neighbors in Venezuela.
The Yanomami commonly eat less than 1 gram of sodium per day.
This study showed that potassium didn’t affect blood pressure when sodium intake was under 6 grams per day.
(So maybe eating all those bananas isn’t relevant in their situation.)
But once you cross that threshold of 6 grams of sodium, potassium intake does matter.

Note the almost linear downward trend in BP as potassium increases in the group that had over 6 grams of sodium chloride per day.
You can see that the fourth quartile of potassium intake in the high-salt population matches the first quartile of the low-salt population.
So it is tempting to see these two graphs as one continuous curve.
The large number of subjects in this study strengthens this correlation.
At 1,285 participants, this study included more people than all others combined.
But this wasn’t an experimental study… This one was strictly observational.
“Our data also signals a graded benefit of higher potassium ingestion. Even small increments in potassium consumption tend to blunt the adverse hemodynamic effects of higher sodium ingestion.”
So why does this occur? What is the theory behind this?
There are at least three theories as to why this happens.
Besides further demonstrating the influence of the sodium/potassium ratio on blood pressure, the study below provides evidence for two potential mechanisms:
This study was notable in that they used subjects in the highest blood pressure range – from 150/90 to 180/115 mmHg – and also a very high amount of potassium.
They gave one group of subjects 3.74 grams of potassium per day and the other group none.
Then they gave each group three different grades of sodium intake and measured their response at each turn.
This study also produced the most unusual-looking graph, yet it is still somewhat intuitive.
I think in the days before color printing became commonplace in journals, I would have stuck with the simple solid/dashed lines to depict each group’s blood pressure…
The weird stippled area makes it look somewhat confusing:
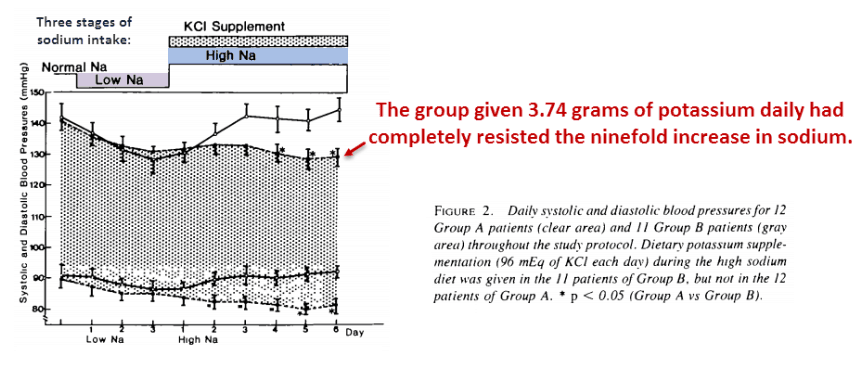
This data is further indication that the sodium/potassium ratio is fundamental in controlling blood pressure…
The high-potassium subjects had lower blood pressure than before…despite the large increases in sodium at the same time.
This goes to show that a 4-gram daily supplement of potassium makes a person highly resistant to the immediate effects of salt.
And the author, Toshiro Fujita, also went the furthest towards trying to explain the mechanism.
As far as I can tell, all explanations for this fall into three categories:
(1) Blood pressure changes induced by catecholamines (again, these are hormones including dopamine, epinephrine, and norepinephrine)
(2) Blood pressure changes consequent of plasma volume
(3) Blood pressure changes via arterial expansion/contraction, such as from nitric oxide
“Although several mechanisms have been demonstrated by which potassium chloride may moderate hypertension, there is still no general agreement as to which mechanism is most likely.”
Fujita was the only one so far to measure norepinephrine concentrations, which did correlate with blood pressure and salt intake.
Catecholamines can increase heart rate.
And since this helps determine blood pressure, it is an intuitive explanation for the effect.
The problem with this explanation, however, is that the changes only occurred when switching dose levels.
After a few days, the catecholamines in both test groups equilibrated – and they converged towards the same point after six days:
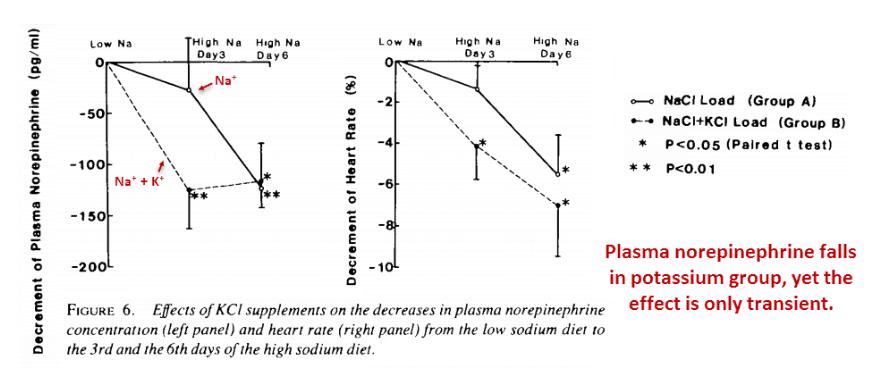
Although plasma norepinephrine paralleled the drop in heart rate, this also falls in the high-sodium group.
Yet Fujita also measured the plasma volume, a parameter that provides perhaps the most intuitive explanation of this effect.
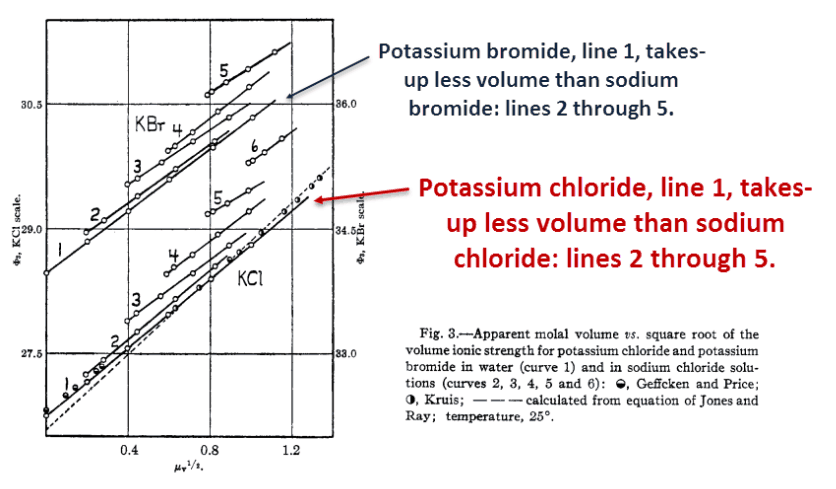
Sodium has a higher osmotic coefficient than potassium.
That means sodium will take up more water in solution than potassium.
Here’s the idea…
Let’s say you put a solution of potassium chloride on one side of a semipermeable membrane and an equal solution of sodium chloride on the other…
You would end up with a higher water level in the sodium half.
“Overall, the increase in blood pressure levels during the high sodium diet correlated directly either with changes in plasma volume or with changes in cardiac output.”
Even though the potassium ion is larger than the sodium ion, water molecules pack more efficiently around it, leading to a higher-density solution.
With the same amount of water, exchanging sodium for potassium would translate into a lower volume.
The potassium supplement blocked the increase in plasma volume induced by salt, just as it blocked the increase in blood pressure.
“The data suggest that the potassium supplement can promote the natriuresis, leading in turn to attenuation of the increase in cardiac output via the suppression of plasma volume expansion, and thus inhibiting the elevation of blood pressure with the sodium chloride load.”
This effect is usually explained by the increase in sodium excretion consequent to potassium intake…
Yet potassium also reduced the volume of solution directly…
This is a classic observation – and is considered a fundamental property of potassium.
Some people would appreciate this mechanism out of simplicity and reliability.
Increased blood volume was also the explanation given by Kijima Iimura, the Japanese scientist who conducted the very first study on this effect in 1981.
“These results suggest that the hypotensive effect of high potassium intake may be caused by reduction of body fluid volume via augmentation of sodium excretion.”
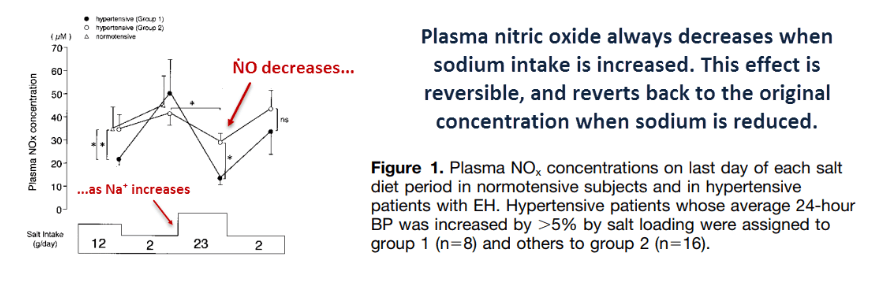
And lastly, there’s the decrease in nitric oxide consequent of sodium ingestion to consider.
There is more information on this than any of the other explanations – perhaps because nitric oxide is so commonly studied.
This is actually a somewhat reliable mechanism, and could very well explain some of the effect.
Small plasma increases of dimethyl arginine – a nitric oxide synthase inhibitor – had also been observed with salt-loading, implying that salt could have initially increased this.
This effect is never mentioned in the media…
And they never focus on potassium because that would imply that people should eat less processed food…
That is a no bueno suggestion for the AMA and the food industries.
The food industry is happy with the AMA suggesting a simple reduction in sodium…
They get to sell “reduced sodium” foods, making themselves appear responsible while not sacrificing much in profit for either party.
Simply taking potassium is much easier than consciously avoiding salt, because some foods – such as cheese and sauerkraut – don’t even exist without salt.
But you never need to worry much about sodium if you are getting enough potassium…
And you don’t even need to know what one gram of sodium looks like…
“Our data indicate that when people have an increased intake of potassium, high intake of sodium is not associated with higher BP.”
Judging by the strength of this evidence, it’s worth considering that this simple mineral works better than overpriced pharmaceutical drugs.
This is actually quite believable, as the sodium/potassium ratio determines blood pressure on the most fundamental level imaginable.
And it could potentially do this in all three ways mentioned above concurrently, all contributing to some degree towards the same effect.
—-Important Message—-
The Easy, Natural Way to Get a Bigger Penis
Most men ask me: “Matt, can I really increase the size of my penis?”
And the answer is yes. Yes, you can.
Most men assume they have to use some weird pumps or take dangerous Big Pharma treatments just to gain a slightly bigger penis…
But not anymore. There’s a better way…
I’ve discovered the easiest way to get a bigger and fatter penis… and it’s natural.
And it really works – by naturally increasing important male hormones such as testosterone and DHT.
You just paint this natural mineral on your penis and watch it grow…

———-

- Fujita, Toshiro. "Hemodynamic and endocrine changes associated with potassium supplementation in sodium-loaded hypertensives." Hypertension (1984) https://pdfs.semanticscholar.org/ebde/58eadf018d1dda3750a1adb57817728ca054.pdf
- Rodrigues, Sérgio Lamêgo. "High potassium intake blunts the effect of elevated sodium intake on blood pressure levels." Journal of the American Society of Hypertension (2014) https://www.ncbi.nlm.nih.gov/pubmed/24524886
- Naismith, Donald. "The effect of low-dose potassium supplementation on blood pressure in apparently healthy volunteers." British Journal of Nutrition (2003): 53-60 https://pdfs.semanticscholar.org/4751/8204b77d3bb5ea6a18b3ae719660d2f511d7.pdf
- Siani, Alfonso. "Controlled trial of long term oral potassium supplements in patients with mild hypertension." British Medical Journal (1987) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1246609/pdf/bmjcred00023-0019.pdf
- Macgregor, Graham. "Moderate potassium supplementation in essential hypertension." The Lancet (1982) https://www.sciencedirect.com/science/article/pii/S0140673682906572
- Sodium: MedlinePlus https://medlineplus.gov/sodium.html
- Sodium https://www.umass.edu/nibble/infofile/sodium.html