
All you need is your hands and a few minutes alone…

—-Important Message—-
This is what I’m doing to last 30 minutes or more with my wife
I’ve discovered a way to boost my lasting power using only my hands…
It feels really, really good and it allows me to last longer and longer every time I do it.
So the next time I go to bed with my wife, I have no problem lasting 30 minutes or more.
And this is huge for me — because I used to be a 5-minute man in bed…
But thanks to this method, now I come when I want to. I have full control.
Here’s what I’m doing to last 30 minutes or more with my wife every single time
———-
Constipation can be fixed by eliminating these gut bugs
Of the hundreds of studies concerning irritable bowel syndrome (IBS), one very consistent trend has emerged:
Methane is highly associated with constipation.
Yet associations don’t necessarily prove causality, and there was previous uncertainty about which occurs first…
Does methane cause constipation, or does constipation promote bacteria which produce methane?
Because methane (CH4) has been long thought physiologically inert, the latter chain of causality had often been assumed true.
However, newer in vitro evidence effectively PROVES that methane causes constipation and not the other way around.
‘In a number of studies in IBS, we have shown that methane is almost universally associated with constipation predominant symptoms in IBS.’ ―Chatterjee, 2007
And sophisticated polymerase chain reaction (PCR) techniques have identified the sole species responsible for producing methane in constipated patients.
On account of this finding, it is now possible to specifically target the specific bacteria responsible using all-natural phytochemicals and herbs.
So taken together, the best science indicates that severe constipation is fundamentally caused by an overgrowth of one microbe, Methanobrevibacter smithii, in either the large or small intestine.
All these associations are quite strong…
They have been reported by scores of researchers from nearly a dozen countries.
There is simply too much evidence to thoroughly summarize in anything shorter than a book, yet below are some highlights from the large body of methane-constipation research:
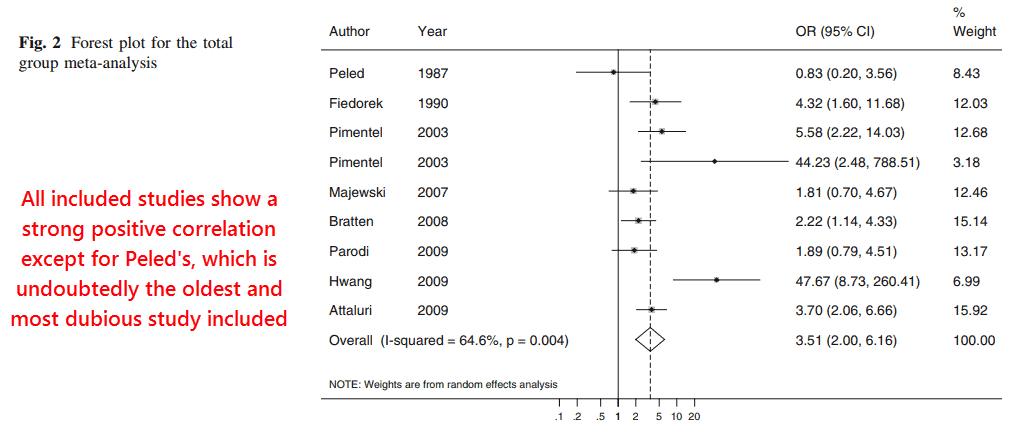
This meta-study identified 44 individual studies on the methane-constipation link published as of 2011, out of which nine were statistically analyzed further.
They could have included many more, really, so this study is by no means comprehensive.
There’s also been dozens of articles published since 2011, and many were excluded for somewhat dubious reasons:
‘Kajs et al. examined methane status and time to first bowel movement after a single meal, an inadequate measure of gut transit to be included in the systematic review.’ ―Kunkel
Trust me, there are far more than just nine studies proving this link.
But despite the small selection, the cumulative result of the chosen studies was highly significant.
Out of the 1,277 subjects comprising the analysis, they had found a methane odds ratio of 3.51 versus constipation.
This means that a “methane producer” — as defined by each individual study’s author — would have a 351% chance of having constipation against chance.
All analyzed studies except one had shown a positive correlation between methane and constipation (Peled, 1985), yet this outlier could easily have been excluded for multiple reasons.
For instance: the Peled study didn’t report at all how it determined constipation…
Yet the Kajs study and one of Pimentel’s were excluded on account of using “non-standard” yet highly objective ways to measure this parameter.
From reading Peled’s study you get the impression he simply asked his subjects whether they felt constipated or not.
Self-reporting of constipation is of course less accurate on account of variable definitions of the term, ranging from once per day to perhaps once a week.
Moreover, people are probably unlikely to relay honest information about that topic.
The association would be even stronger had they forgone the underpowered and crude Peled study and included others.
Yet the cumulative odds ratio is probably not the best way to view the strength of association anyhow.
This is because each study uses its own criteria of what defines a “methane producer.”
Definitions range from 1 parts per million methane in the breath (Peled, 1987) all the way up to 20 parts per million (Pimentel, 2003).
All people have M. smithii in their intestines and also produce methane (Dridi, 2009), yet only about 36 to 50% of these have levels high enough to be detected in expired breath (Pimentel, 2003).
The degree of constipation also varies immensely. Since both variables lie on a spectrum and vary individually, the best way to compare their relationship is probably through Pearson coefficients.
This fortunately was done by a few researchers (Soares, 2005; Lee, 2012), including a study by Soumya Chatterjee which is very comprehensive:
This study took IBS patients with constipation and plotted their breath methane concentrations against their constipation scores.
Two measures of constipation were used:
- A value from 0 to 100 that represents perceived constipation severity over the entire week
- The more objective count of total eliminations per day.
Both constipation indices were graphed against breath methane taken within the first few hours and graphed without a cut-off value.
Most other studies used bar graphs comparing “producers” against “non-producers,” but this is better because it reveals methane’s concentration dependent effect:
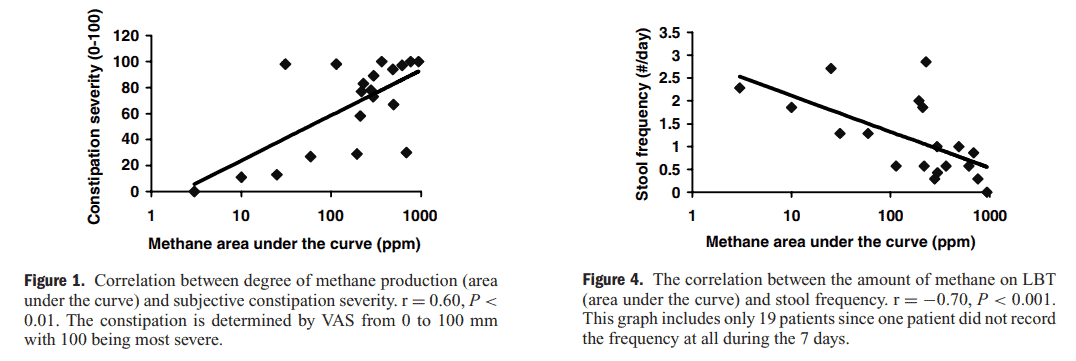
As you’d probably expect, the more objective measure of constipation bears a stronger relationship to methane than the more subjective one (r = −.70 vs. r = .60).
When breath methane increases so does constipation (r = .60).
And total breath methane, and thus constipation, has an inverse relationship to frequency (r = −.70).
In other words: the more methane a person produces, the fewer times they eliminate per day.
‘Methane on LBT is associated with constipation both subjectively and objectively. The degree of methane production on breath test appears related to the degree of constipation.’ ―Chatterjee, 2007
Pearson coefficients having a value of unity, and negative unity, represent a perfect straight line through all data points (r = ±1).
Although values of .60 and −.70 are quite respectable, and would be considered strong correlations by most, there’s reasons you’d actually not expect a more perfect fit in this circumstance.
This is because lactulose absorption varies individually and the timeframe used was short.
Breath methane concentrations were sampled over just three hours.
Methane emissions over this timeframe are consistent with the time lactulose arrives the small intestine, not the colon.
There’s a good amount of evidence to infer that some methane producers have M. smithii overgrowth in the colon, not the small intestine, and would only expire large amounts of CH4 after about 10 hours or so.
‘The CH4 concentrations were significantly higher in the delayed transit group than in the normal transit group between 0 and 135 min, which indicated the time interval of the small bowel or the proximal colon.’ ―Lee, 2012
For instance, the Peled study reported that 15⁄18 (.83%) of his “methane producers” had become “methane non-producers” after bowel cleansing as a preliminary to colonoscopy.
Of course this would be indicative of M. smithii in the large intestine, not in the small one.
The only study that’d examined breath methane over an extended timeframe had shown a spike in some patients 10½ hours after the lactulose was administered (Cloarec, 1990):
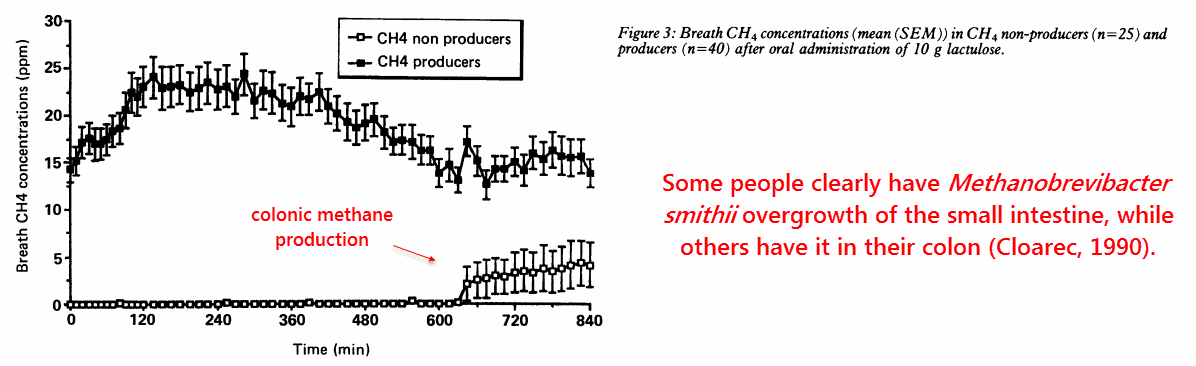
Besides using the lowest cut-off point out of any study, a mere 1 part per million methane, the Peled study determined basal CH4 concentrations.
Every other study besides Fiedorek’s measured methane within three hours after administering lactulose (or glucose), perhaps why the Peled study was the only to report a negative correlation.
Another assumption that had perennially obscured the link between methane and constipation was the idea that M. smithii only populates the left colon. While this is probably the natural state of affairs, M. smithii has now been shown capable of colonizing the entire digestive tract of rats under certain diets (Mathur, 2012).
This strain is now presumed to inhabit nearly the entire digestive tract of humans.
The other classic myth was also proven false, twice. Once in 2005 and again in 2012.
Methane most certainly CAUSES constipation and is not merely a consequence of it:
This had been a three-pronged study involving surgically modified dogs, living humans, and explanted intestines from guinea pigs (ileum).
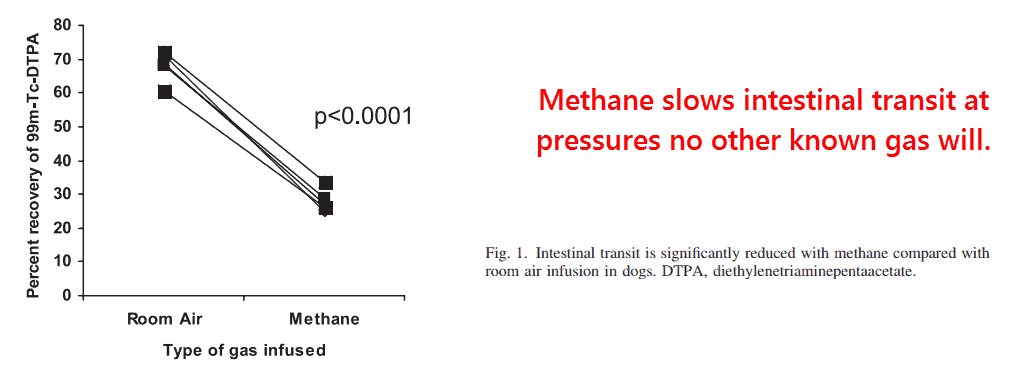
The substudy using dogs had isolated an intestinal segment using two inflatable balloons. Between this sealed-off segment, methane was infused and transit determined using radioactive tracers.
The researchers had found, as compared to room air, that methane would cause a 59% reduction in intestinal velocity.
‘Luminal methane infusion reduced radioactive marker recovery in all five dogs compared with room air by an average of 59%.’ ―Pimentel, 2005
This is significant, especially considering that no other gas known will do this. Hydrogen (H2) however appears to act the other direction, to INCREASE transit, and hydrogen sulfide (H2S) is implicated in the conditions of high-motility such as Crohn’s and ulcerative colitis.
Carbon dioxide (CO2), oxygen (O2), and nitrogen (N2) are of course all inert by comparison and presumed safe.
Although nitric oxide (ṄO), nitrosonium (NO+), and hypochlorite (ClO−) can certainly cause cancer they aren’t known to cause constipation.
Results in humans were just as incriminating for methane.
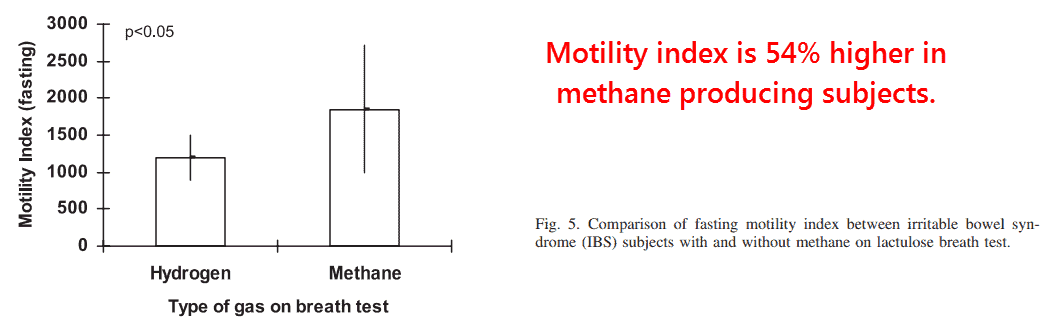
The motility index in methane producing subjects was significantly higher than in the non-methane subjects (1,851 versus 1,199).
The motility index is determined by summing the time until excretion so carries a somewhat paradoxical name.
Because the motility index increases as transit time increases, it should rightly be called “the non-motility index” or “the constipation rating.”
The substudy on explanted guinea pig intestine may seem strange at first, and this is because methane actually INCREASED the muscle’s contraction force.
The same thing was reported in the human subjects.
It may seem at odds that methane — a general anesthetic — would slow nerve velocity yet somehow increase muscle contraction, an effect mediated through nerves, but the next study sheds light on this issue:
This is the only other article besides the one by Pimentel, shown above, that reports effects of methane when applied directly.
Incidentally, this is because the FDA will not allow exogenous methane to be infused into humans on account of its flammability (Chatterjee, 2007).
This study had also used guinea pig intestine, so it is actually just like the previous one except for a few important details.
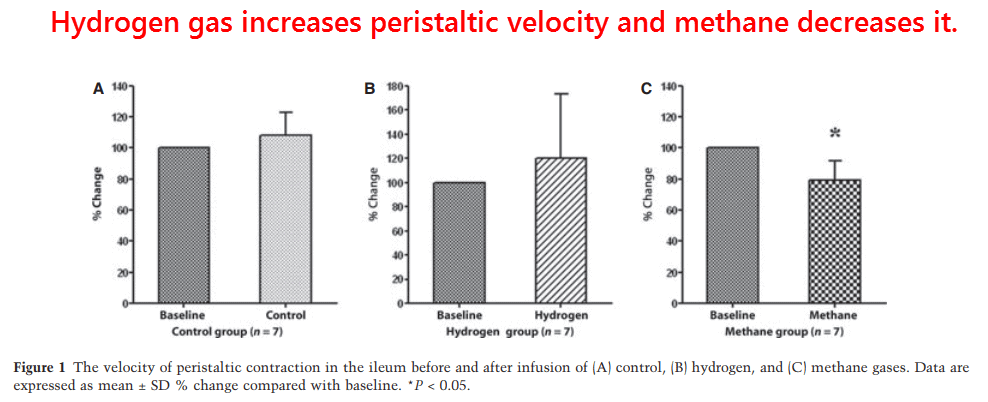
This study used hydrogen (H2) in addition to methane (CH4), isolated the entire digestive tract and not just the ileum, and most importantly determined the peristaltic velocity.
The muscles which line the intestines in rings are serially activated in waves, the speed of which is the peristaltic velocity.
Pimentel had measured peristaltic velocity as well, albeit indirectly, when he recorded the transit time of the tracer in dogs.
This study, however, placed pressure transducers every 2.5 centimeters along the entire length of the intestine and measured peristaltic velocity directly.
They found the expected: methane decreased the velocity of the peristaltic wave while hydrogen increased it:
Others showed the same effect with hydrogen (Pimentel, 2003), which perhaps could increase motility simply by displacing methane.
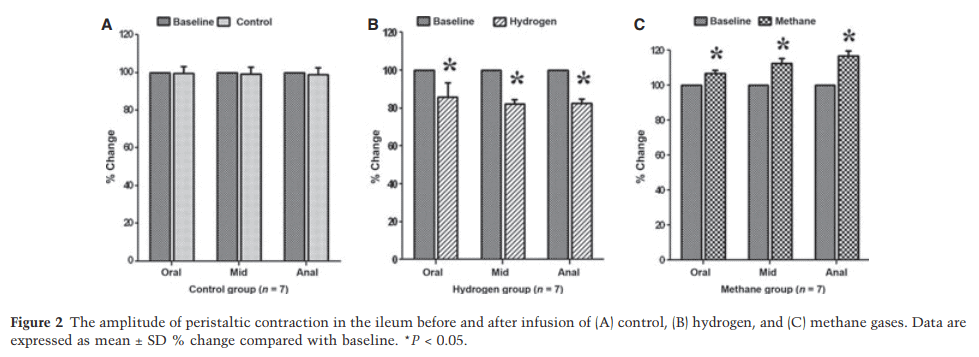
This study also confirmed the increased contractile force following methane administration, another effect reversed by hydrogen:
Methane is unreactive and doesn’t have a receptor, two facts which leave its mechanism of action wide-open.
This nonreactivity and potency of general anesthetics is in fact a classic dilemma…
They’ve always had an “officially unexplained” mechanism of action.
‘Their chemical properties are such that it is impossible to believe that they produce narcosis by taking part in chemical reactions involving the formation and breaking of ordinary chemical bonds. Moreover […] these substances, with the exception of a few (nitrous oxide, carbon dioxide, chloroform), would not be expected to form even weak hydrogen bonds, and we may call them the non-hydrogen-bonding anesthetic agents.’ ―Pauling, 1961
Newer data reveals that general anesthetics, such as methane, slow nerve conduction by intercalating into nerves and disrupting Förster resonance energy transfer (Hameroff, 2002).
This seems the most plausible way to explain methane’s effects on peristaltic waves and motility, but what about the contractile force?
Muscle contraction appears most fundamentally caused by calcium ions (Ca2+) interacting with tropomyosin and “crosslinking” it (Ebashi, 1968).
Calcium is known to interact with microtubules, or individual nerve fibers, and could be repelled from them the moment photo-electronic impulses flow through them.
Perhaps methane is displacing calcium from nerves, thus enhancing contraction, at the same time it impedes nerve velocity by quenching microtubule fluorescence?
Yet it’s not necessary to know exactly how this effect occurs to be certain that it does. The methane and constipation link the most consistent finding to emerge out of all IBS studies to date, and the relationship is so strong you can consider methane as being the prime cause.
In fact, breath methane concentration is the most accurate test for constipation so far conceived-of (Hwang, 2009).
‘When methane was used to predict the assignment of C-IBS [constipation type IBS] compared to non-C-IBS, it had a sensitivity of 91.7% and a specificity of 81.3%.’ ―Hwang, 2009
New accurate PCR studies indicate that M. smithii is the sole cause of methane in humans (Kim, 2012), a gas which also increases body weight (Basseri, 2012), so it’s probably safe to assume this strain should be the target.
Upcoming articles will explain the reasons for M. smithii overgrowth, what you can eat to reduce it, and what natural treatments you can use to eradicate it.
—-Important Message—-
Men: if you’re not having 2 or more bowel movements a day, your erections may be suffering…
The penis and prostate are right next to the bowel in the male body.
So when food collects and ferments there, it shoots out dangerous endotoxins that poison the manhood!
That’s why I developed a simple protocol that restores penile functioning and gets a man’s libido sky high.
It is really simple to do and gets great results for most men, often within a week.
Here’s how you can get it for free and heal your gut and penis all in one
———-

Jahng, J. "The effects of methane and hydrogen gases produced by enteric bacteria on ileal motility and colonic transit time." Neurogastroenterology & Motility (2012) http://hmphanmi.com.cn/hmp/upload/event/study_6/6.pdf
Pimentel, Mark. "Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity." American Journal of Physiology-Gastrointestinal and Liver Physiology (2006) https://pdfs.semanticscholar.org/0fc2/3577d2371f15a12e6708d56d7903182299be.pdf
Cloarec, D. "Breath hydrogen response to lactulose in healthy subjects: relationship to methane producing status." Gut (1990) https://gut.bmj.com/content/gutjnl/31/3/300.full.pdf
Chatterjee, Soumya. "The degree of breath methane production in IBS correlates with the severity of constipation." The American journal of gastroenterology (2007) https://www.nature.com/articles/ajg2007154
Kunkel, David. "Methane on breath testing is associated with constipation: a systematic review and meta-analysis." Digestive diseases and sciences (2011) http://hmphanmi.com.cn/hmp/upload/event/study_6/4.pdf