
It’s NOT the caffeine and it’s NOT the magnesium…

—-Important Message for Men Who Want Perfect Blood Sugar—-
The zipcodes where nobody gets diabetes — how men in certain cities have stopped and EVEN reversed diabetes in an unusual way
In these secret zip codes, men easily eat sugar and yet they have no diabetes, no pre-diabetes, no blood sugar problems…
While around them, blood sugar is shooting up — causing an epidemic in rockiness-killing diabetes.
What’s going on in these zip codes? Why do these men living in these cities have literally zero diabetes?
———-
NEW discovery: this ingredient in coffee has HUGE benefits
According to the CDC, treatments for blood sugar problems rank sixth among “treatable conditions” and account for an average annual cost of $5,000 per patient.
While this news may sound favorable to Pfizer and Merck executives, this is a considerable amount of money to spend only for treatments with side-effects.
From a patients’ perspective, I think most would agree that preventing blood sugar problems by drinking coffee would be preferable to taking metformin and Rosiglitazone — on the basis of taste alone, if not for the cost & convenience.
But side-effects aside, is coffee really as effective as the treatments currently prescribed for blood sugar problems?
The answer to this question is, quite surprisingly, a unanimous & resounding YES!
Epidemiological studies consistently report dose-dependent reductions in prevalence with increasing coffee intake…
…and 3 of coffee’s main components have been experimentally confirmed as anti-diabetic agents in both humans & mice.
And even more surprisingly, none of coffee’s 3 main anti-diabetic substances are caffeine.
All this evidence has been published and verified twice-over, yet it remains little-known among the general population and probably just ignored by doctors — they don’t want all their drug money going to Starbucks®.
The main protective effect of coffee in diabetes had been uncovered in the 1960s, yet it wasn’t until recently that the final pieces of the puzzle had been set in place.
Now It is finally known how coffee achieves its effects.
So if you’d like to be diabetes-free and have extraordinary glucose control, then keep reading. Out of space considerations, just a fraction of the evidence is given below:
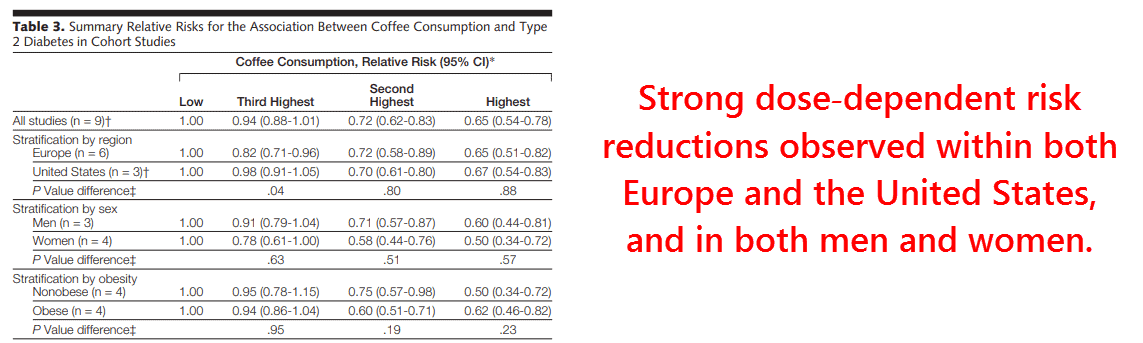
These authors examined all outstanding data on coffee vs. diabetes risk, eventually compiling the results of 9 studies, including 193,473 participants total.
The results were shocking, with risk ratios ranging from .94 in the lowest consumption group to .65 in the highest:
Similar risk ratios are also found in Japan, a country that consumes predominantly filtered coffee.
Because Scandanavians primarily drink boiled coffee, this demonstrates that the effect persists regardless of brewing method.
This effectively eliminates kahweol and cafestol from consideration, 2 diterpenes found only in non-filtered coffees.
These are crude risk ratios, and they get even stronger after adjustments for other lifestyle factors.
This is because coffee drinking also correlates with lower leisure, less physical activity, and the consumption of donuts and pastries:
“This is of importance, as higher coffee consumption tends to be associated with cigarette smoking,21-23,25,33 lower leisure physical activity,21-23,25,33 and an unfavorable diet,21,25 and adjustment for lifestyle factors generally strengthened the inverse association between coffee consumption and type 2 diabetes.21,23,24,33” ―van Dam, 2005
Some epidemiological studies have effectively ruled-out magnesium and caffeine through statistical methods, as well as the potential confounding effects of the aforementioned lifestyle considerations.
And because it’s so counterintuitive that caffeine isn’t at all responsible for this effect, it’s perhaps best to present evidence showing that explicitly:
Although not quite as large as the 193,473 person meta-analysis above, this one here is close with 41,934 men and 84,276 women.
What this study lacks in breadth and scope, as compared to the meta-analysis, is more than compensated by the additional insight gained through its statistical methods.
After adjusting for such things as: age, total caloric intake, family history of diabetes, polyunsaturated fatty acids, magnesium, body mass index, and physical activity, the protective effect was revealed as being even greater than before:
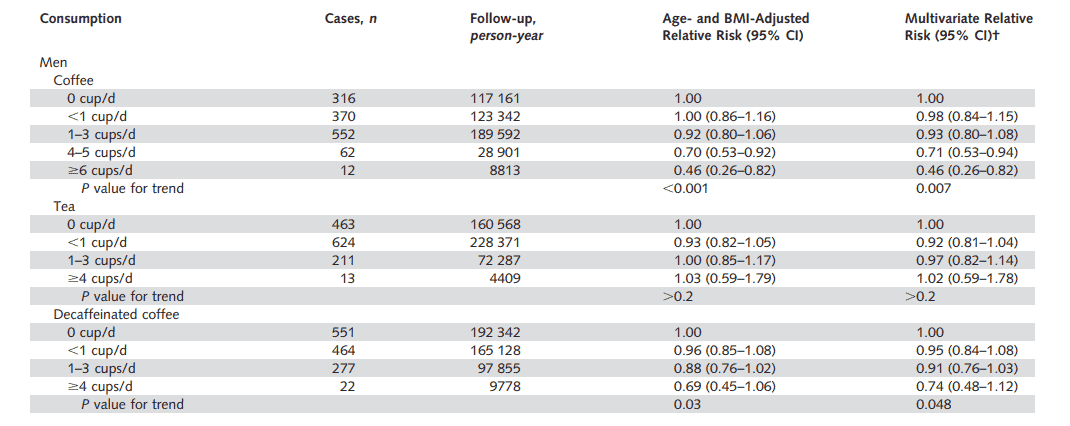
Risk ratios had ranged from .98 for 1 cup per day drinkers, to .46 in those consuming more than 6 cups.
So after eliminating most relevant confounders, it’s seen that 1 daily pot of coffee will cut the risk of diabetes by half.
This effect was absent in tea drinkers, a finding also reported by others.
The effect also persisted with decaffeinated coffee, an effect supported by experimental studies showing caffeine to actually increase insulin resistance.
Yet the regular consumption of caffeine abolishes its ability to release catecholamines, which are the cause of the insulin resistance it produces.
This “tolerance effect” occurs only after about 7 days of routine use.
So even though it’d be logical to believe that caffeine has a net pro-metabolic effect that’s uncovered after it stops releasing catecholamines — e.g. after the drinker gains tolerance — the epidemiological data nonetheless indicates that decaffeinated and regular coffees have roughly the same effect.
“In our study, the statistically significant inverse association for coffee persisted even after adjustment for magnesium intake.” ―Salazar‐Martinez, 2004
There is also experimental evidence showing that decaffeinated coffee is just as effective as the regular caffeinated variety in improving the glucose response, effectively leaving little doubt as to its non-importance.
This study above had also eliminated magnesium after adjusting for its intake, which despite having an undeniable anti-diabetic effect only exists in brewed coffee at ~7 milligrams per cup — a nearly insignificant amount.
So if it’s not the caffeine, and if it’s not the magnesium, then what exactly is it?
The question has plagued researchers for decades, and for this reason we now have some answers.
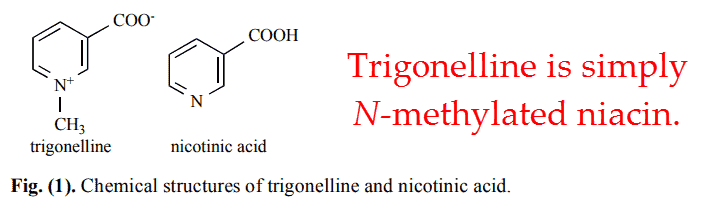
The anti-diabetic effect of coffee is perhaps best explained by 1 compound, trigonelline, with 2 others being of secondary importance.
Trigonelline was first isolated in 1887 in Germany and its name derives directly from Trigonella foenum-graecum, the Linnaean name for fenugreek.
A century later it was discovered in coffee where it’s found in concentrations 10 times greater than those in fenugreek:
Green coffee beans have the highest amounts of trigonelline, ranging from 1 to 3% dry mass.
Trigonelline is progressively converted during roasting into niacin and methane, which evaporates, so light roasts contain more than dark ones.
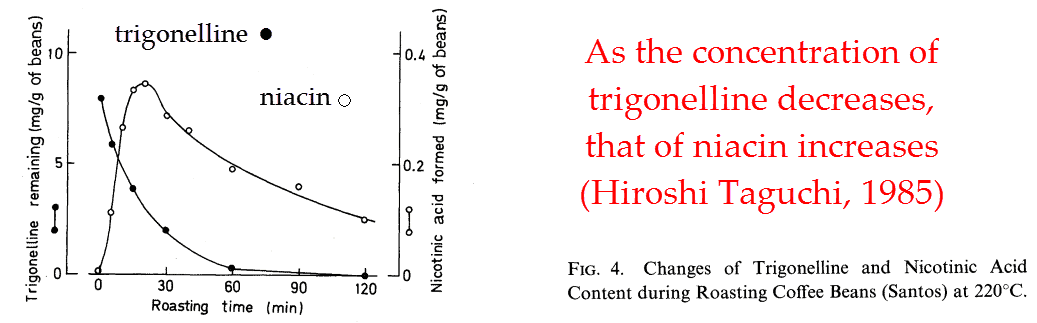
Nevertheless, what remains is always more trigonelline than niacin.
Taking the average of 6 coffees commercially available, you could expect 61mg trigonelline per cup and 5.1mg of niacin.
This value is remarkably consistent among different types, with 72mg reported in instant coffee per cup and 74mg in espresso.
So you may wonder, why is trigonelline important? Why would this be more effective than niacin, a B vitamin?
There are at least 2 reasons for this, 1 being a necessary consequence of its methyl group.
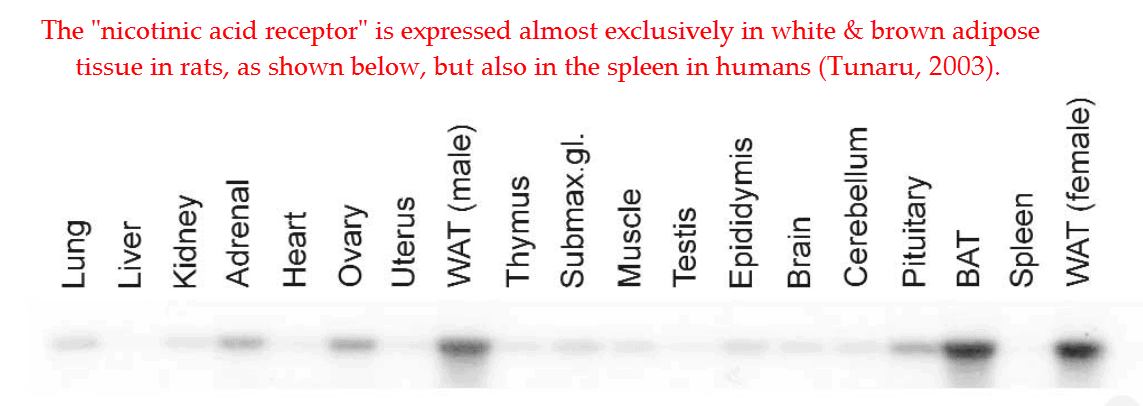
Niacin has long been used clinically to decrease plasma free fatty acids, an effect now known to be mediated through HM74a receptor activation.
This same receptor is also called PUMA-G in rats, and knockout studies prove that it’s responsible for niacin’s anti-diabetic effects.
Originally known as the “nicotinic acid receptor,” the now-called HM74a is thought to normally respond to β-hydroxybutyrate — a ketone body — and not niacin.
This is because nicotinic acid doesn’t naturally exist in concentrations high enough to activate this receptor, despite having an 8 times greater affinity for it.
Niacin at normal intakes is converted into niacinamide, an analogue completely inactive on HM74a.
For this reason and a few more, you cannot directly extrapolate vitamin B6 contents from food charts into their antidiabetic activity.
Beta-hydroxybutyrate on the other hand can be found circulating at its receptor EC50 concentration after only 1 day of fasting.
Since the HM74a receptor is found primarily in adipose tissue where it inhibits lipolysis and fatty acid release, it makes sense that β-hydroxybutyrate should be its endogenous ligand.
This is because ketone bodies are: (1) originally derived from fatty acids, (2) are a main circulating energy source during fasting, and (3) should provide a feedback inhibition on their own production.
It was known during the ’60s that the intravenous administration of ketones will lower plasma glucose and free fatty acids, and β-hydroxybutyrate will do both.
So this is almost certainly how niacin and trigonelline decrease plasma free fatty acids, with the latter being more potent simply because it’s not quickly metabolized into niacinamide.
But also, niacin is known to cause a “rebound effect” that eventually increases plasma free fatty acids upon chronic use. This enigmatic effect is never properly explained, but it could have something to do with the depletion of the methyl pool…
Niacin is excreted largely as N-methylnicotinamide, the formation of which progressively steals methyl groups from the body over time.
Regardless of how this happens, the rebound effect doesn’t appear mediated through the HM74a receptor because it doesn’t occur with acipimox — a synthetic ligand.
And because trigonelline already has an N-methyl group, you wouldn’t expect a rebound effect from that either.
This would be consistent with the epidemiological data on coffee intake versus diabetes, with chronic users having the lowest rates.
The hypoglycemic effect of trigonelline had been reported over a half-century ago, and it’s now assumed responsible for the anti-diabetic effect of fenugreek.
So if you already drink a few cups of coffee per day, fenugreek supplements should have less effect than they would otherwise.
Here is some evidence demonstrating the anti-diabetic potential of trigonelline, comparing it head-to-head against niacin:
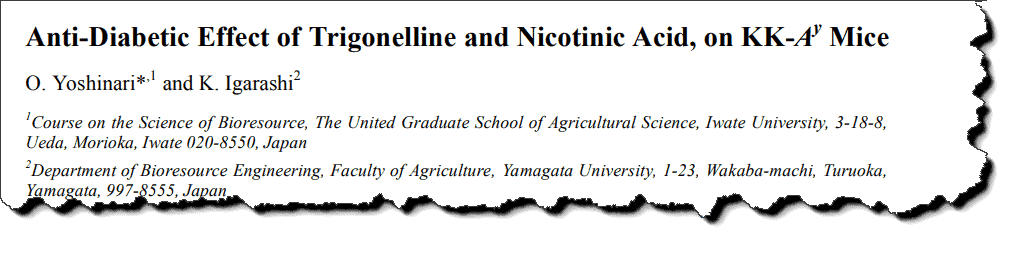
In this study, diabetic mice were given either trigonelline or an equimolar amount of niacin for 28 days.
So after 1 month, each rat had their basal blood chemistry analyzed and were subjected to an oral glucose tolerance test.
The results plainly show that both niacin and trigonelline are veritable antidiabetic agents, and similar enough in structure & effect to assume they have near-identical mechanisms of action:
So even though trigonelline has never been tested on the HM74a receptor, enough circumstantial evidence exists to assume that it activates it.
It has been shown that 5-methyl- and 6-methylnicotinic acid can activate HM74a in nanomolar concentrations but trigonelline, synonymous with 1-methyl- or N-methylnicotinic acid, surprisingly hadn’t been tested.
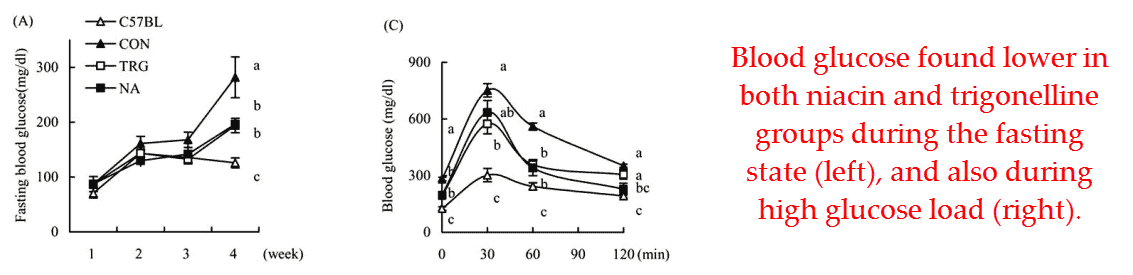
This same effect had also been demonstrated by the same researchers previously with Goto-Kahizaki rats, an animal that better highlights the difference between trigonelline and niacin:
The glucose response was greater with trigonelline than with niacin, and only the former had maintained a reduction in plasma free fatty acids after 43 days.
So trigonelline is better than niacin because it doesn’t deplete the methyl pool, yet this may not explain completely the anti-diabetic effects of coffee.
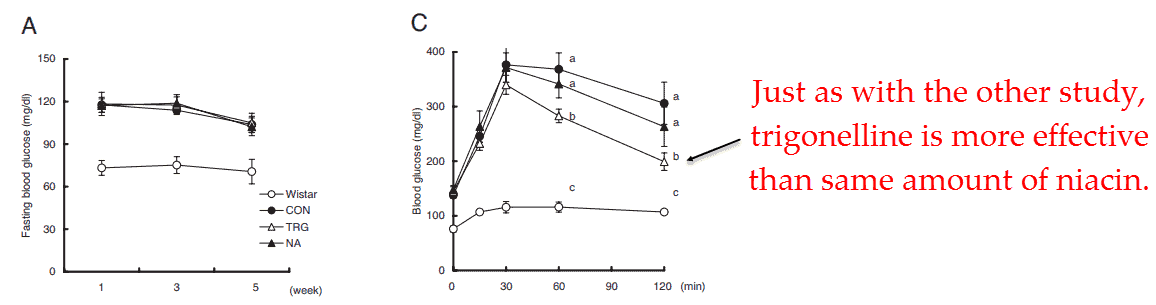
This is because coffee also contains substantial amounts of chlorogenic acid, an anti-diabetic molecule in its own right.
Chlorogenic acid has been shown to delay blood glucose increases in vivo, and also Na+-dependent glucose transport across intestinal membranes in vitro.
Chlorogenic acid also causes a change in the incretin profile consistent with delayed glucose uptake in humans. Since phlorizen induces a near-identical response, all evidence is consistent with chlorogenic acid being an SGLT-1 inhibitor.
So besides inhibiting lipolysis through trigonelline, the chlorogenic acid also found in coffee delays glucose uptake from meals.
So perhaps those donuts aren’t so bad…as long as you have coffee of course.
Chlorogenic acid is “broken down” more quickly upon roasting than caffeine or trigonelline, yet just as with the latter it’s fortuitously converted into yet another useful compound.
Chlorogenic acid becomes 4-caffeoylquinide, a veritable anti-opiate nearly on par with naloxone in potency.
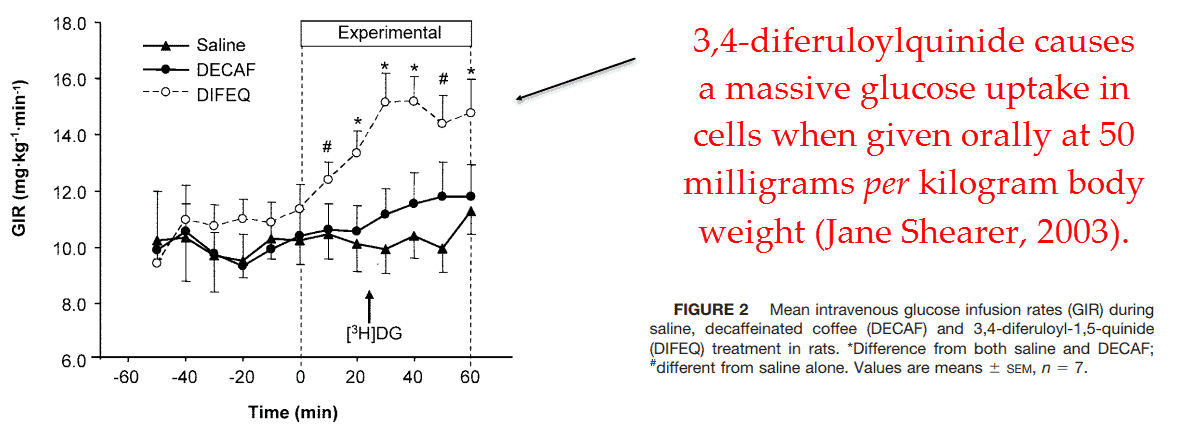
A very similar molecule found in roasted coffee called 3,4-diferuloylquinide has also been shown to radically increase the glucose infusion rate, e.g. the amount of infused glucose required to maintain its steady state concentration.
This molecule is also a μ-opioid receptor antagonist, perhaps implying that opiates may affect glucose metabolism. No other biological targets of coffee quinides have been reported.
Yet despite their alarming effects, anti-opiate coffee quinides exist in concentrations only at ¼ that of chlorogenic acid, yet this of course varies greatly by roast level.
Although quite provocative, the anti-opiate quinides have been studied the very least among all active coffee components.
There isn’t much to go on besides just 1 cross-over study comparing the glucose response between light and dark roasts.
Yet since the subjects were required to abstain from caffeine before the trial and also during the interim washout period, the results are confounded by the hyperglycemia caused by caffeine-induced catecholamine release.
As mentioned earlier, coffee ceases to release catecholamines after just 1 week of routine use. This is great in many ways, but makes it difficult to compare studies involving chronic coffee drinkers to those involving coffee-naïve subjects.
So until a study is published that tests all of coffee’s anti-diabetic components in isolation and in relevant concentration ranges, their relative contributions towards coffee’s anti-diabetic effect will remain debatable.
Regardless of how they should be ranked, coffee does contain at least 4 experimentally confirmed anti-diabetic compounds:
- Trigonelline ≈ 40 to 110 milligrams per cup (Ludwig & Clifford, 2014)
- Chlorogenic Acid ≈ 6 to 188 milligrams per cup (Ludwig & Mena, 2014)
- anti-Opiate Quinides ≈ 52 milligrams per cup (de Paulis, 2003)
- Magnesium ≈ 7 to 24 milligrams per cup (Ludwig & Clifford, 2014)
So perhaps it takes consuming all 4 compounds to achieve the ½ reduction in diabetes risk, and then of course only after the caffeine-induced catecholamine effect wears-off.
—-Important Message From Our Sponsor—-
7 simple techniques to having any woman you want

You’ll be happy to know that this is not a gimmick…
The techniques I’m about to share with you are REAL.
In fact, they are based on the most cutting-edge female psychology discoveries — and they’ll get girls begging to be with you, starting tonight.
———-