
Can smoking really help boost a man’s T?

—-Important Message—-
How to unclog your penile chambers from this dangerous toxic build-up
I’ve discovered a dangerous toxin that is building up in men’s members…
It comes from certain foods, certain pollutants in the environment…it’s almost impossible to avoid…
And it’s clogging up the arteries and leading to terrible blood flow, especially down there…
And when blood flow isn’t good, erections isn’t good either…
In fact, erections suffers tremendously when blood flow is poor.
It’s the #1 reason why men stop getting good erections — and most men have no idea the root cause is this dangerous toxic build-up.
Fortunately, I’ve discovered an easy way to get rid of this toxin and clear the build-up for better blood flow and better rockiness.
Use this to wash the penile chambers clean — you can sip it in the morning or at night
———-
Hidden benefits of smoking — what they’ll never tell you
First of all I’m not advising you to smoke a pack of cigarettes every day. But you should read this carefully even if you do NOT smoke.
As you may know, Europeans have been smoking tobacco since 1492, and Native Americans centuries before that.
Exactly how long the Natives have been smoking tobacco cannot be known with certainty due to their lack of a written language.
Any mention of negative health effects went largely unreported prior to the 18th century, a time coinciding with introduction of ammonia and hypochlorite-bleached paper to tobacco products.
This new paper is why only cigarettes have been linked to cancer, and not cigars or pipe tobacco.
Ammonia is added to increase pH and hence nicotine volatility.
This could almost be seen as a good thing, were it not for ammonia (NH3) converting into nitric oxide upon combustion (Miller, 1983).
Nitric oxide (ṄO) is a well-known carcinogen and should be avoided, yet ammonia-free tobacco is now available online.
[1] NH3 + acidic nicotine ⟶ NH4+ + basic nicotine
[2] NH4+ + ³⁄₂O2 + ΔH ⟶ ṄO + 2H2O
And whatever ammonia isn’t pyrolyzed by the flame — i.e. becomes nitric oxide — can potentially be volatilized and inhaled.
In high concentrations, ammonia is a toxin in its own right, and hyperammonemia is largely responsible for the inebriation seen during liver failure.
Hypochlorite is also an established carcinogen used in paper manufacturing.
There have been epidemiological studies conducted showing an increased prevalence of certain cancers in paper mill workers (Torén, 1991), and this was not correlated with smoking or with sulfur dioxide — another paper-bleaching agent (Jäpplnen, 1987).
And yet: smoking has actually been shown consistently protective against certain types of cancers, namely those of the breast and uterus in females (Terry, 2002). These are the two main estrogen-dependent cancers, and the lower cancer rates in smokers is commonly explained by tobacco’s antiestrogenic effect.
Female smokers had been shown to have lower estrogen concentrations in literally dozens of studies, and there are now even review articles on that (Baron, 1990).
Male smokers have also been shown to have lower estrogen levels (Small, 1985), yet their naturally low estradiol concentrations approach the limit of detection in assays (Dai, 1988).
This fact introduces noise — uncertainty — and is why the results have been so variable.
‘The inconsistent findings of a relation between cigarette smoking and estradiol concentrations might be due to the relative unreliability of the estrogen measurements in men, since the concentrations of estrogen in the serum are so low that they are very close to the detection limit for the radioimmunoassay.’ ―Dai
Yet just as consistent as the antiestrogenic effect of tobacco in females is its ability to increase androgens in both sexes, most notably DHEA and androstenedione.
The fact that tobacco can reliably decrease estrogens yet increase androgens implies that aromatase was inhibited, an effect tobacco smoke has been shown to do (Osawa, 1990).
So if a person can avoid ammonia-adulterated tobacco, use natural unbleached paper, supplement γ-tocopherol, and take vitamin C they should be able to use tobacco with little or no risk to their health.
Natural tobacco is certainly safer than most of Big PHarma’s treatments, no doubt, and also less harmful than many foods.
Tobacco use tends towards an androgen-heavy steroid profile, on average, and without the expected increase in estrogens stemming from the precursor effect.
‘Nonsmokers had significantly lower testosterone and androstenedione concentrations than smokers.’ ―Dai
These androgenic effects of tobacco are most likely a consequence of its ability to stimulate corticosteroid synthesis:
This study was an offshoot of a larger one: the 22,071 person Physicians Health Study conducted to examine health outcomes between aspirin and β-carotene supplementation.
A subset of 543 males were selected whose blood was on-file, a healthy subgroup that also served as controls to compare against cardiovascular disease cases.
‘…several studies have found higher levels of DHEAS among cigarette smokers (2,4,7,8).’ ―Salvini
So this group was healthy, by definition, and nothing was wrong with them.
So all these researchers really did, in essence, was to measure plasma DHEA concentrations in pre-drawn blood samples and correlate them with smoking history previously recorded.
They took into consideration over ten parameters, yet found only two significant positive correlations to DHEA levels: that to drinking (+.07), and that to smoking (+.16).
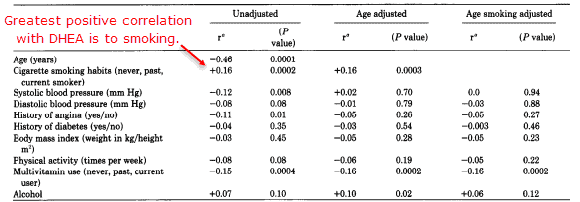
And not surprisingly, age was shown to have the strongest effect.
Age was also the strongest negative correlation, yet the strongest positive one was to smoking.
Smoking was also the second strongest correlation, in either direction, and right behind the reduction of adrenocorticoids seen with age.
‘The present study confirms and strengthens these findings since it is based on a large (n = 543) number of healthy subjects.’ ―Salvini
Seeing as the smokers had more dehydroepiandrosterone (DHEA) in their plasma, let us see if the translates into more androstenedione as you might predict:
This study initially had 2,300 men, out of which 1,709 were compliant with the interview and measurements.
After excluding cigar and pipe smokers for being unclassifiable — i.e. neither truly “cigarette smokers” or “nonsmokers” — and eliminating other people based on incomplete data, they were left with a still-substantial group of 1,241 men.
They took into account age, waist-to-hip ratio, BMI, cigarettes smoked, DHEA, androstenedione, testosterone, DHT, and cortisol.
As with the previous study, the second greatest correlation they found between any two parameters — right behind age vs DHEA — was between androgens and smoking.
Although smoking was also positively correlated to DHEA (r = .14), the most significant correlation was to androstenedione (r = .26).
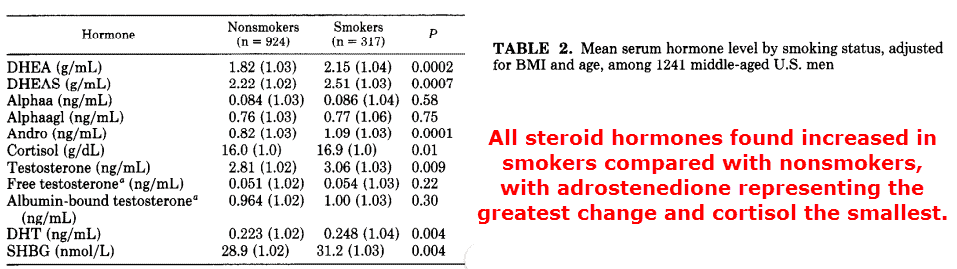
Dehydroepiandrosterone sulfate, testosterone, and DHT were also found to be increased in smokers when compared to nonsmokers.
‘Compared with nonsmokers and independent of relative weight and age, cigarette smokers had increased serum levels of DHEA (18% higher), DHEAS (13% higher), cortisol (5% higher), androstenedione (33% higher), testosterone (9% higher), DHT (14% higher), and SHBG (8% higher).’ ―Field
Free testosterone was also increased in smokers, and this was despite a concomitant increase in sex hormone-binding globulin (SHBG) — a serum protein that binds free androgens.
Every steroid hormone downstream of DHEA was increased in this study, and especially the androgens.
Cortisol, a stress hormone, showed the lowest increase at 5%.
So these are very consistent effects, and explained by others as an increased response to adrenocorticotropin (Hautanen, 1993).
Corticotropin is released by the pituitary and is how the brain controls the amount of corticosteroids released by the adrenal glands.
Cortisol release is how a traffic jam, or rude person, can directly influence your biochemistry.
This increased adrenal output was truly an androgen-heavy response, with much less increase of cortisol observed.
This effect was explained by Finish chemists as probably being the result of 11β-hydroxylase inhibition.
So smoking initially increases androgens through increasing precursor DHEA, yet also potentiates the same effect by reducing how much DHEA becomes cortisol and corticosterone (Hautanen, 1993).
‘These results suggest that smoking decreases the activity of either 21- or 11β-hydroxylase in the adrenal cortex, which results in increased secretion of adrenal androgens.’ ―Hautanen
So the convincing epidemiological evidence cannot be brushed aside by imagining that “more manly males choose to smoke,” or something to that effect.
The nature of the increase in androgens with smoking has been proven experimentally to be causal, and not simply the result of a personality choice.
This effect also occurs in females (Khaw, 1988), perhaps making them a bit more independent.
Propaganda expert Edward Bernays renamed cigarettes as “torches of freedom” while marketing them to women in the ’20s.
Most people seem to view this event more-or-less as “a shameless advertising ploy,” yet perhaps there’s a bit of truth to that on account of the pro-androgenic effect of tobacco.
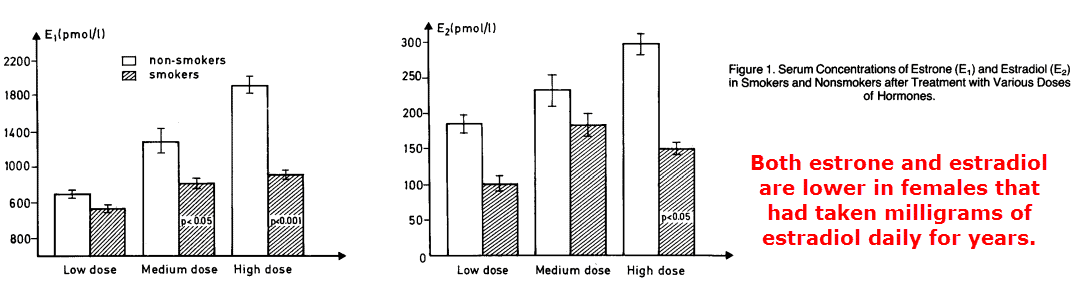
Smoking also radically lowers estrogen in females, an effect most conspicuous in those taking supplemental estradiol in milligram-sized doses (Jensen, 1985):
This makes a person wonder whether or not males could expect lower estrogen from smoking.
Women have the very same aromatase enzymes as males do, they only have more of them.
Smoking is notorious for lowering estrogens in females, and from that you might assume it would in men as well.
Although testosterone outnumbers estradiol about 30∶1 in males, on average, there are cases where estrogen can increase and then exert an inimical influence:
Gynecomastia and central obesity, for instance, are somewhat estrogen-dependent.
While it seems most accurate to view gynecomastia as being caused by prolactin, estradiol is responsible for transcribing the prolactin receptor through ERα.
So without estrogens acting beforehand, prolactin can do nothing besides mimic growth hormone at its eponymous receptor.
‘In contrast, the response of 17-hydroxyprogesterone, dehydroepiandrosterone, and androstenedione to ACTH was higher in smokers than non-smokers, while the increase in cortisol was of marginal significance.’ ―Hautanen
But luckily for anyone curious, it does appear that this effect has been examined: male smokers have been shown not to have an increase in estrogens despite an increase in androstenedione and testosterone, precursors for estrone and estradiol.
This is unexpected, as the ratio of androgens to estrogens remains more-or-less constant in males regardless of the absolute testosterone concentration.
Whenever you see an increase in androgens, a corresponding increase of estrogens usually follows.
Having more androstenedione and testosterone also means there’s a greater substrate availability for aromatase, the only enzyme which can convert them into estrone and estradiol.
This study was a spin-off of the Multiple Risk Factor Intervention Trial (MRFIT): a naive attempt to reduce cardiovascular disease by reducing cholesterol, tobacco, and salt.
That is simply not the way to go about things: Omega-6 fatty acids and vitamin C intake were more correlated with cardiovascular disease than salt or cholesterol, and both have very plausible biochemical mechanisms behind them.
This article actually contained the results of two studies, yet both measuring roughly the same parameters.
A longitudinal study composed of 121 men, total, while a case-control study consisted of 163 cases and 163 controls.
This makes for 447 participants all told, quite a bit more than most others conducted on this topic.
Moreover, they used a considerably more accurate technique for determining steroid hormones than any other:
‘Sex hormone concentrations were determined by a highly specific method involving extraction, column chromatography, and radioimmunoassay using a specific antibody.’ ―Dai
This is important because some studies showed a slight increase in estrogens while others reported a decrease.
Yet all of the studies besides this one simply used radioimmunoassay on whole plasma, by itself, and never had anyone else separated the individual hormones beforehand via chromatography.
Because male estrogen levels approach the limit of detection for the radioimmunoassay, the most common way to detect them, having other steroids present in the plasma could lead to significant interference.
It would certainly seem as if this study gives the most reliable data on estrogen levels in smokers, which basically didn’t change a bit despite more androgens:
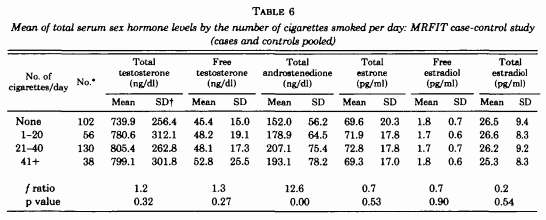
All androgens increased in a dose-dependent manner until reaching over two packs per day, after which there was just a slight decrease compared to the intermediate group. This group however only included 38 out of the 326 people, and there’s probably something else going on when a person decides to smoke that much.
The heavy smokers (41+) still had more androgens than the “light smokers” (1 to 20), who in turn had more than nonsmokers.
The group with the highest androgens smoked between 21 and 40 cigarettes per day.
‘There was a strong positive association between cigarettes/day and serum total testosterone level and between cigarette smoking and serum total androstenedione level . Nonsmokers had significantly lower testosterone and androstenedione concentrations than smokers.’ ―Dai
There was essentially no difference in either estradiol or estrogen levels in smokers, a reassuring observation when noting the large sample size studied and more accurate chemical techniques.
Smoking apparently prevents androgen conversion into estrogens by inhibiting aromatase, an effect it has consistently been shown to accomplish.
The aromatase inhibition of tobacco was known since 1986 (Barbieri, 1986), and then confirmed independently — and unintentionally — four years later (Osawa, 1990).
The researchers of the latter study noticed that cigarette smoking before biochemical work influenced the results.
The chemists even admitted to smoking in the lab in their article, a less-common practice these days:
‘In the process of developing a simple and sensitive method for routine assays of aromatase activity, we realized that a puff of cigarette smoke during pipetting greatly influenced the outcome of the experiment. By eliminating smoking in the laboratory area, we were able to carry the original project to completion. However, the nagging question of why tobacco smoke affected aromatase activity eventually led to the investigation not only of cigarette smoke, but also tobacco leaves and several purified components of tobacco extracts…’ ―Osawa
And since that time — in a newer study — aromatase inhibition by nicotine was demonstrated in monkeys, in their brains, confirmed via PET scan.
—-Important Message For Men Who Don’t Like Smoking—-
Drinking this Tee soup slows down aromatase — boosts natural testosterone while lowering harmful estrogen

Many men don’t have a problem producing testosterone.
Not even in men in their 50s, 60s, 70s, and beyond.
The real problem is a process called aromatization that speeds up as a man ages…
With aromatization, testosterone is being created but getting turned into estrogen.
And that’s the problem — too much testosterone is getting turned into estrogen.
So T levels go down and estrogen levels go up!
But when you drink this 2-minute Tee soup I’ve discovered, you slow down aromatase…
So testosterone STAYS testosterone — and your T levels shoot upwards while estrogen falls back down.
Here’s how to make my Tee Soup at home — free recipe
———-

Salvini, Simonetta. "Effects of age, smoking and vitamins on plasma DHEAS levels: a cross-sectional study in men." The Journal of Clinical Endocrinology & Metabolism (1992) http://academic.oup.com/jcem/article-abstract/74/1/139/2652983
Field, Alison. "The relation of smoking, age, relative weight, and dietary intake to serum adrenal steroids, sex hormones, and sex hormone-binding globulin in middle-aged men." The Journal of Clinical Endocrinology & Metabolism (1994) http://academic.oup.com/jcem/article-abstract/79/5/1310/2649238
Dai, W. S. "Cigarette smoking and serum sex hormones in men." American journal of epidemiology (1988) http://academic.oup.com/aje/article-abstract/128/4/796/131764
Osawa, Yoshio. "Aromatase inhibitors in cigarette smoke, tobacco leaves and other plants." Journal of enzyme inhibition (1990) http://tandfonline.com/doi/abs/10.3109/14756369009040741
Barbieri, Robert. "Nicotine, cotinine, and anabasine inhibit aromatase in human trophoblast in vitro." The Journal of clinical investigation (1986) https://dm5migu4zj3pb.cloudfront.net/manuscripts/112000/112494/JCI86112494.pdf